

Why this summer sets your 2028 Star Rating, not this October's
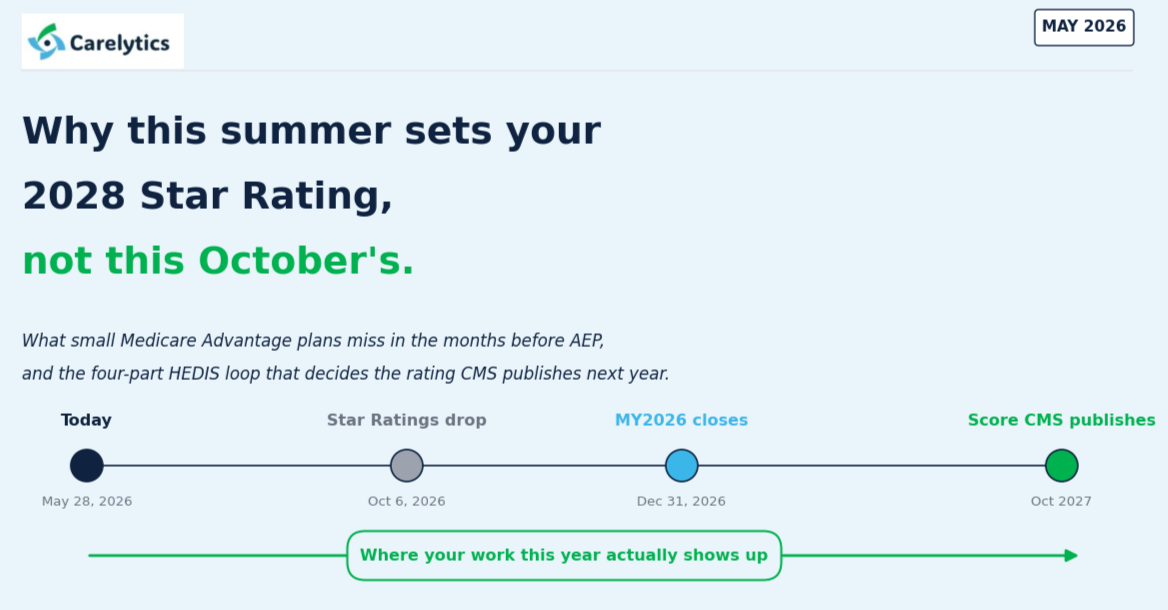
What small Medicare Advantage plans miss in the months before AEP, and the four-part HEDIS loop that decides the rating CMS publishes next year.
1. The benchmark gap small plans live with
Bids hit submit this week. ANOCs go out September 30. Marketing materials are approved through August. AEP opens October 15. Between June and October, a small or mid-sized Medicare Advantage plan has about 14 weeks of operational freedom. Most of it gets spent on desk-review responses, call-center training, and material approvals.
What rarely gets spent on: a serious look at how the plan stacks up against the 10 to 30 other plans a member sees side-by-side on Medicare.gov in October. Most large plans run that benchmark monthly, whereas many small plans submit, mail, and hope. Hence, this blog is focused on small plans.
2. The benchmark sheet you should have on the wall
Seven metrics, one page, every county you operate in: monthly premium, the in-network MOOP cap, member out-of-pocket for a typical 5-day inpatient stay, the same for a 20-day SNF rehab stay, the same for an annual Part B visit basket, total episode out-of-pocket, and Star Rating. The county median for each. Where you sit on each. That is the sheet.
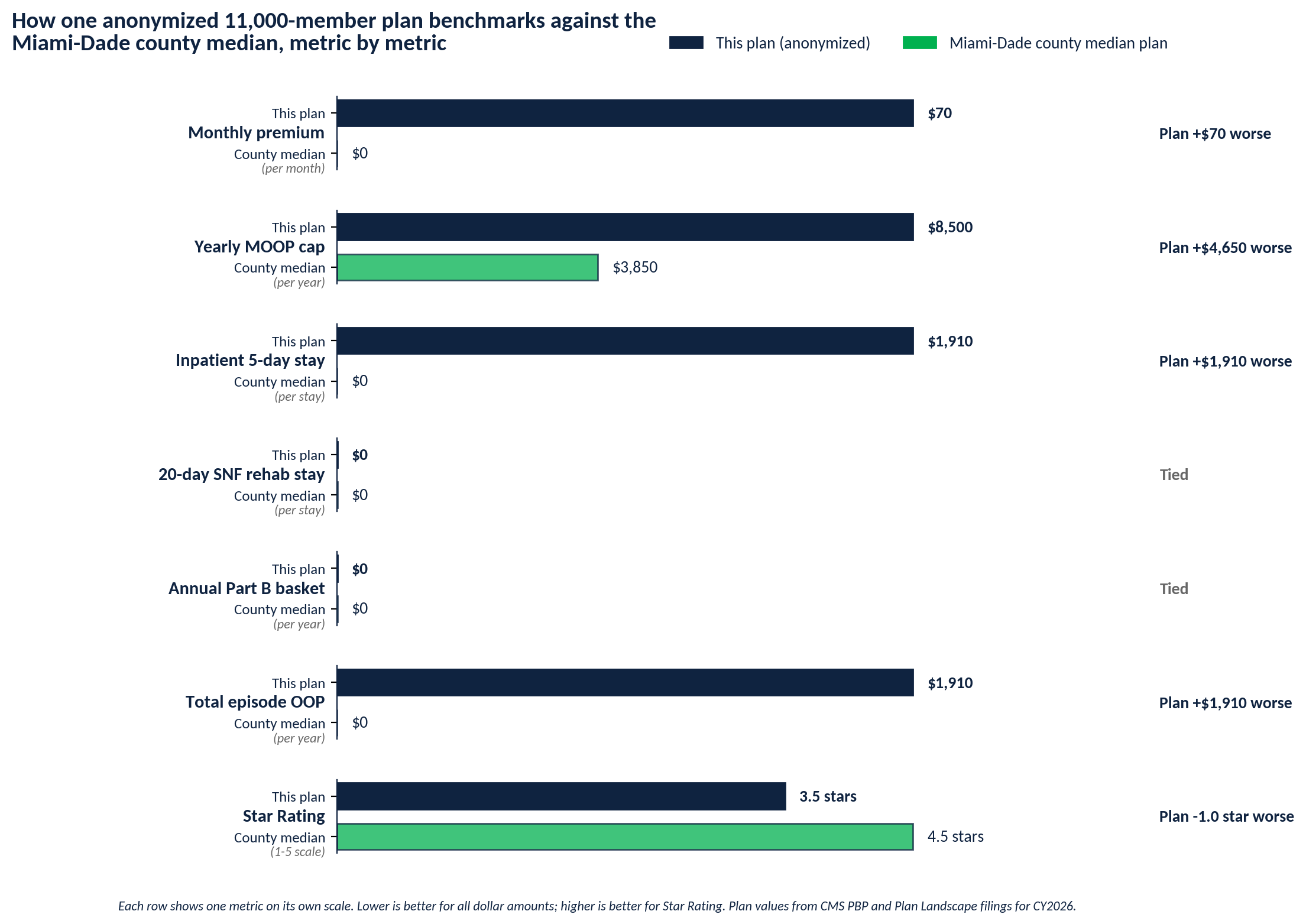
Figure 1: The plan against the Miami-Dade county median across seven metrics members see on Medicare.gov. Five metrics worse, two tied. The plan does not know it
The plan in Figure 1 is real, anonymized. Its members compare it to 36 other MA-PD plans during AEP. Five of the seven visible metrics fall short of the county median. The plan will be surprised by Q1 attrition. It was not the market. It was the sheet they never built.
3. What to do with the six "locked" metrics before October
Six of the seven metrics are baked into the bid you just filed. They cannot move for CY2027. But each one still unlocks four decisions you can act on between June and October.
A. Communication strategy
If your premium sits $30 above the county median, your call center, brokers, and marketing team all need a counter-narrative by July: which strengths do you lead with, which supplemental benefits do you put up front, which network claims do you defend. A plan that goes into AEP without these gets compared to median and loses.
B. ANOC pre-emption
The Annual Notice of Change goes to current members by September 30. A plan that knows its members will see a premium or MOOP gap can shape the ANOC to lead with what stayed the same or improved, and pre-empt the comparison shop. The ANOC is the most under-used retention tool small plans have.
C. Broker channel briefing
Most small-plan acquisition runs through brokers. Brokers compare plans the same way Medicare.gov does. A plan that briefs its broker channel in August with specific positioning on weak metrics gets defended at the kitchen table in October. A plan that does not gets dropped from the broker's shortlist.
D. CY2028 bid input
This is the highest-leverage use of the sheet. If you sit below median on five of seven metrics this AEP, your CY2028 bid planning starts in July, not next April. Where can you trim premium without breaking margin? Which supplemental benefits cost least per point of preference? Which counties did you misprice? The work to answer takes nine months.
4. The hidden lever inside the sheet
Of the seven metrics, six are operational inputs as described above. Star Rating is different. The score CMS publishes on October 6 of this year reflects measurement year 2025 data, which closed five months ago and cannot move. But the score CMS publishes in October 2027, which will set your CY2028 Quality Bonus Payment, worth roughly $500K to $2M per 0.5 stars on a 30,000-member plan, depends entirely on what plans do between now and December 31. That is the lever most small plans leave on the floor. They wait for the October release to learn how they placed, then react. The plans that win the next cycle work it during the measurement year, not after.
5. Where Star Ratings actually come from
Roughly 60 percent of the Part C summary rating comes from clinical HEDIS measures: Controlling High Blood Pressure (CBP), Breast Cancer Screening (BCS-E), Colorectal Cancer Screening (COL-E), medication adherence, diabetes care. Each one is a closable gap on a specific list of members. The remaining 40 percent comes from CAHPS member experience and HOS health outcome surveys. Those are slower to move, but HEDIS gaps can be closed in weeks if you know who the right members are and how to reach them.
6. The four-part loop most HEDIS vendors do not close
KNOW which gaps are open. REACH the right members through channels they actually use. CLOSE the gap through scheduled action. PROVE the closure to CMS through NCQA-compliant supplemental data. That is the full loop. Incumbents like Inovalon, Cotiviti, and Episource stop at KNOW, and stop late. Their gap reports run on quarterly batch cycles. By the time you know who needs a colonoscopy, half the measurement year is gone.
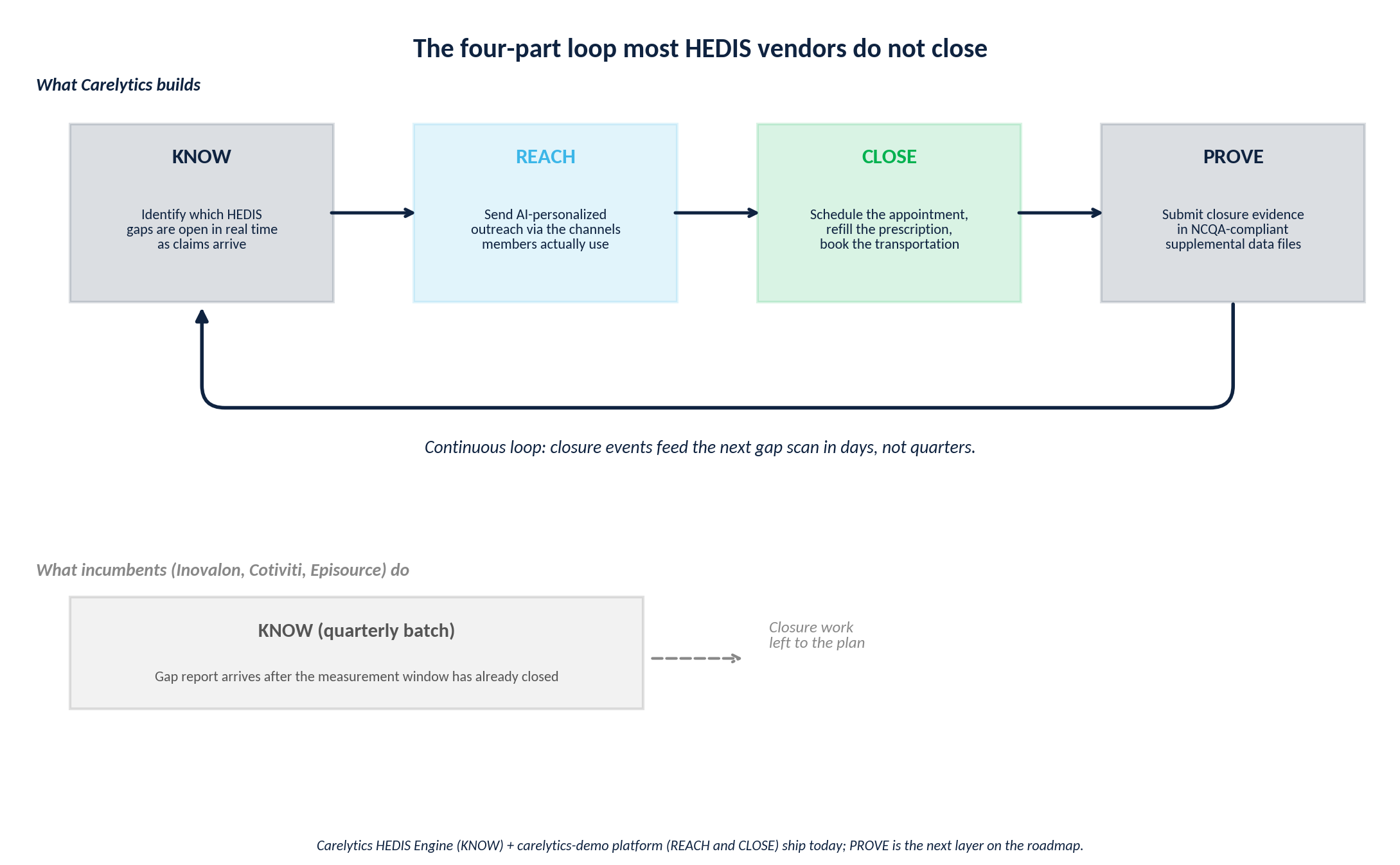
Figure 2: The continuous loop, contrasted with the quarterly batch step incumbents stop at.
7. How Carelytics closes the loop today
Carelytics is three production capabilities and one roadmap layer.
The Benchmark Report is the diagnostic that opens the loop. The benchmark chart in Figure 1 is something Carelytics produces for any contract in any county where you operate. It surfaces the metrics where you sit below median, names the three to five gaps that are most likely to drive AEP attrition, and feeds the prioritization logic of the HEDIS engine below. Available as a one-shot diagnostic or as a continuous monthly refresh. This is where conversations start with most plans.
The HEDIS Engine is the KNOW layer. Carelytics’ deterministic rules engine built on NCQA HEDIS MY 2026 data. 87 measures are fully encoded. Risk-adjusted utilization O/E ratios are computed for all 10 RAU measures, including Plan All-Cause Readmissions and ED Utilization. Python and SQLite, fully deterministic, every gap call auditable for NCQA review. Updates as claims arrive, not as quarters close.
The Member Engagement Platform is the REACH and CLOSE layer. A member-facing web app and SMS channel, our platform MARPLES lets members chat to schedule appointments, request prescription refills through a live Walgreens integration, and book transportation. A care-manager dashboard with searchable rosters, intervention timelines, and cohort analytics. The intervention engine processes each member profile against open HEDIS gaps and decides between direct message, add to campaign, create new campaign, or no action. Every decision is logged with token cost and reasoning. Human-in-loop approval before execution. Cloudflare serverless deployment auto-scales for plans of any size.
8. What to do this summer
There are two parallel lanes of summer work, on different timelines. Most small plans run one and miss the other.
Lane 1: CY2027 AEP preparation (14 weeks)
Mid-June: run the benchmark sheet for every county you operate in and identify where you sit below median.
July: write the communication strategy and brief the broker channel.
August: counter-position weak metrics in marketing materials.
September 30: ANOC mails to current members.
October 15: AEP opens; you defend on your strengths and acknowledge your weak spots.
Lane 2: CY2028 Star Rating work (7 months)
Mid-June: identify the three HEDIS measures most dragging your projected MY2026 score.
Early July: pull closable cohorts, members with one open gap on a high-weight measure who are still in the measurement window.
July through December: REACH and CLOSE campaigns, by SMS for under-65 dual eligibles, by app for actively engaged members, by phone outreach for the rest.
December 31: MY2026 closes. The work that lands inside it sets your October 2027 score, your CY2028 QBP, and your CY2028 Medicare.gov display.
9. Next Steps
If the benchmark sheet in Figure 1 looks like your county, the conversation is short. Email contact@carelyticsllc.com for a sample benchmark report for a county you operate in. We will send back the benchmark chart for one of your contracts and a list of the three measures we would prioritize closing between now and October.
Ready to see where your plan stands before October? Carelytics runs a free benchmark analysis for any MA contract — we'll show you exactly which HEDIS gaps are costing you stars and which members are still closable before MY2026 ends.